Solitary fibrofolliculoma on the nasal septum: a case report
Article information

Abstract
Fibrofolliculoma is a benign, perifollicular, connective tissue tumor that usually arises in the form of multiple lesions; it is rarely seen as a solitary lesion. The lesions are clinically asymptomatic, 2 to 4 mm skin-colored, soft dome-shaped papules. Here, we report a patient who visited our hospital with a palpable lesion on the nasal septum. The lesion did not cause pain upon palpation, and nasal endoscopy confirmed an irregular wart-like lesion measuring 6 × 6 mm in the left anterior nasal septum near the columella. Other otolaryngology findings were normal, and there were no similar lesions in other parts of the body. None of the patient’s family members were known to have had such lesions. An excisional biopsy was performed on the mass for removal of the lesion, and histological examination confirmed the lesion as fibrofolliculoma. We report the first case of solitary fibrofolliculoma in the nasal septum in a healthy 62-year-old woman along with a review of the relevant literature.
INTRODUCTION
Fibrofolliculoma is an autosomal-dominant benign tumor characteristically found with Birt-Hogg-Dubé syndrome. The lesions are clinically asymptomatic, skin-colored, soft dome-shaped papules measuring 2 to 4 mm. Fibrofolliculoma was first described by Birt et al. [1]. It occurs mainly in the form of multiple lesions in adults in various areas, such as the scalp, forehead, face, and neck [2,3]. Solitary fibrofolliculoma is very rare [4,5]. To the best of our knowledge, this is the first report of a case arising from the nasal septum [6]. Here, we report the clinical features and results of surgical treatment of a rare isolated fibrofolliculoma located on the left nasal septum in a 62-year-old woman, along with a review of the relevant literature.
CASE REPORT
A 62-year-old woman visited our hospital, as an outpatient, with a palpable lesion on the left nasal septum. The patient visited us after recommendation of surgical removal at a local hospital. The lesion did not cause pain upon palpation while physical examination was performed. Nasal endoscopy confirmed an irregular wart-like lesion in the left anterior nasal septum near the columella (Fig. 1). Other otolaryngology findings were normal, and there were no similar lesions in other parts of the body. None of the patient’s family members were known to have had such lesions. An excisional biopsy was performed on the mass for removal of the lesion and histological confirmation. The lesion, measuring 6× 6 mm, was completely resected with iris scissors under local anesthesia (Fig. 1). Visually, the mass showed no invasion into the cartilage or other tissues, and no adhesion to the periphery. A permanent biopsy was requested for the resected mass.

A 62-year-old woman visited with a palpable lesion on the left nasal septum. (A) Nasal endoscopic findings of mass located in the anterior nasal septum near the nasal columella. (B) A whitish-gray wart-like mass measuring 6×6 mm was excised. (C) Appearance at 6 months postoperatively showing the nasal septum, with no recurrence.
Histological examination revealed fibrofolliculoma showing cystically dilated hair follicles with thin proliferating epithelial strands emanating from them. The strands are surrounded by perifollicular fibrous tissue and show little cellular atypia (Fig. 2). Based on these pathological results, a fibrofolliculoma was confirmed. We reexamined the patient’s skin on the face, neck, axillae, upper trunk, and groin, but there were no specific findings. The patient had no family history of multiple skin papules or any skin diseases. Therefore, a solitary fibrofolliculoma was diagnosed. There was no recurrence of the lesion over 6 months of follow-up after surgery (Fig. 1).
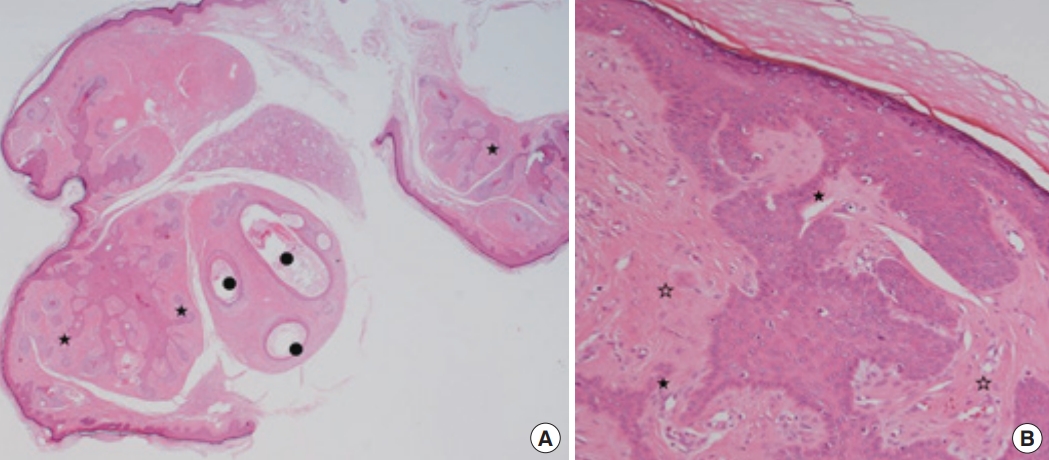
Histopathological photograph showing a fibrofolliculoma. (A) Low-power appearance. Cystically dilated hair follicles (black bullets) with thin proliferating epithelial strands (black asterisks) emanating from them (hematoxylin and eosin stain, × 20). (B) High-power appearance. Proliferating epithelial strands (black asterisks) with little cellular atypia surrounded by dense fibrotic stroma (empty asterisks) (hematoxylin and eosin stain, × 200).
DISCUSSION
Fibrofolliculoma can be associated with multiple fibrofolliculoma as a part of Birt-Hogg-Dubé syndrome and may occur as a solitary benign lesion although few cases have been reported. This benign tumor occurs mainly in adults in the form of multiple lesions on various areas, including the scalp, forehead, face, and neck [1]. Multiple lesions generally appear after the age of 25 and show autosomal-dominant inheritance, but sporadic cases have also been reported [7]. However, solitary fibrofolliculoma is very rare compared to multiple lesions, shows no heritability, and is not associated with other skin abnormalities [4]. There have been very few subsequent case reports. To the best of our knowledge, only 14 cases have been reported to date, of which three occurred in the nose [5]. All three developed from skin of the nose. No cases in the nasal septum have previously been reported, and to the best of our knowledge, this is the first case of solitary fibrofolliculoma in the nasal septum described to date [3,4,6].
The average age of onset of solitary fibrofolliculoma is over 50 years [1,8], in contrast to the multiple hereditary form with onset at a significantly earlier age [1,2,9]. However, there is no gender predominance [5]. Our patient was also a woman in her sixties, with no genetic predisposition or other skin diseases.
Solitary fibrofolliculoma can present with a variety of clinical manifestations without the typical recognizable local or systemic symptoms, and appear as yellow-white or skin-colored, smooth, dome-shaped lesions measuring 2 to 4 mm. Most cases are asymptomatic, although cases with bleeding and itching have been reported [2,10]. Our case was asymptomatic, with a rather large wart-shaped lesion measuring 6 × 6 mm with no pain on palpation. Solitary fibrofolliculoma is usually diagnosed through histopathological examination after excisional biopsy due to its clinical similarity to other lesions [11]. Our case also had no local or systemic symptoms, and was confirmed pathologically after excisional biopsy.
Diagnosis of fibrofolliculomas can be difficult, because patients have no recognizable or systemic symptoms and fibrofolliculomas are similar in appearance to other benign tumors formed in hair follicles [5]. Also, solitary fibrofolliculomas are very rare and the diagnosis is made only after histological examination is done. For these reasons, a solitary fibrofolliculoma may lead to misdiagnosis and undertreatment. The diagnosis for all lesions is made histologically, based on the characteristic findings of occasionally dilated hair follicles containing keratinous material surrounded by a moderately well circumscribed thick mantle of fibrous tissue. The infundibular follicular epithelium extended out into this fibrous mantle forming epithelial strands or cords.
Due to its rarity, there is no consensus regarding the optimal treatment and prognosis of solitary fibrofolliculoma. Although known as a benign mass, complete resection of solitary fibrofolliculoma is considered desirable [5]. All patients reported to date have been treated by shaving or complete resection biopsy. In our case, treatment was performed by complete excisional biopsy, and meticulous surgical procedure was required to prevent the injury to the nasal septal cartilage which can induce septal perforation or saddle nose. There has been no relapse to date over 6 months after surgery.
Here, we reported the first case of solitary fibrofolliculoma in the nasal septum in an otherwise healthy 62-year-old woman with no other skin lesions or relevant family history, along with a review of the literature.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Ethical approval
This report was approved by the Institutional Review Board of Busan Saint Mary’s Hospital (IRB No. BSM 2023-03).
Patient consent
The patient provided written informed consent for the publication and use of her images.
Author contributions
Conceptualization: Soo Kweon Koo. Data curation: Young Hoon Chi, Joo Young Woo. Visualization: Hyuni Son. Writing - original draft: Young Hoon Chi. Writing - review & editing: Tae Kyung Koh, Soo Kweon Koo. Resources: Joo Young Woo, Hyuni Son. Supervision: Tae Kyung Koh, Soo Kweon Koo. Validation: Tae Kyung Koh, Soo Kweon Koo.