

DISTAL MOBILE FRAMEWORKS: THE ALAR CARTILAGE AND ABUTMENTS (NASAL TIP-SUPPORTING STRUCTURES)
Alar cartilage (lower lateral cartilage)
The alar cartilage is also known as the lower lateral cartilage or the tip cartilage. While the alar cartilage, especially the middle and medial crura, is smaller and less developed in Asians, it exists on a wide spectrum of variation among individuals, even within a single race (Fig. 1). Due to the high demand for prominent tip projection with a weak cartilaginous framework in Asians, it is challenging to obtain satisfying results using only the suture technique. Therefore, additional manipulation of the alar cartilage is usually required to obtain movability for projection or lengthening by releasing fibrous attachments around it, aside from using suture techniques [1].
Anatomy of the alar cartilage
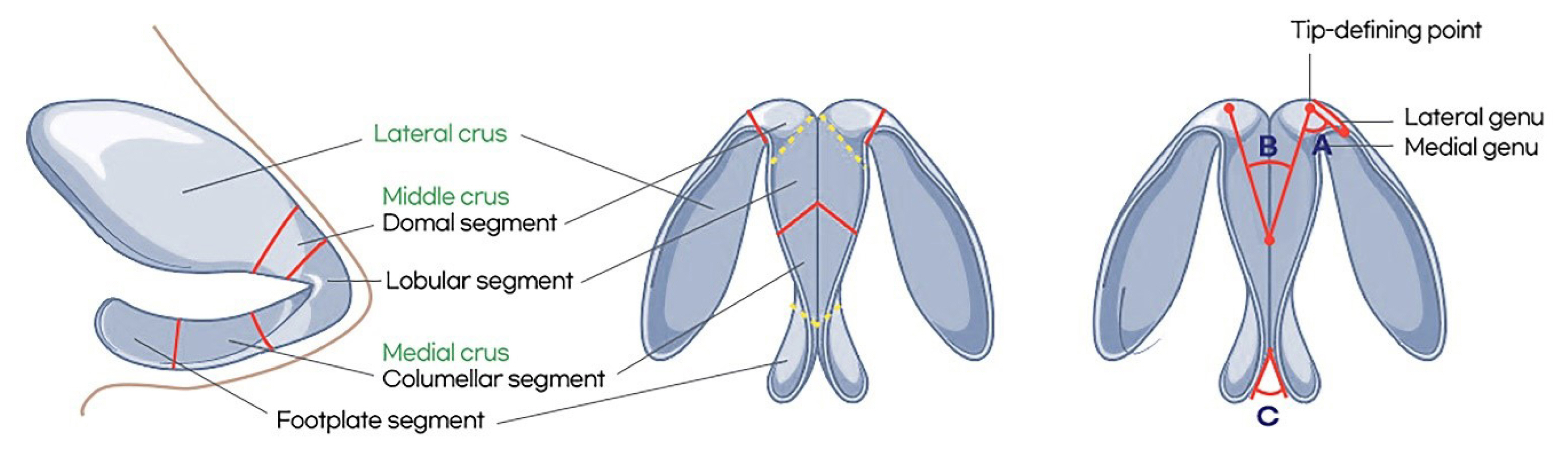
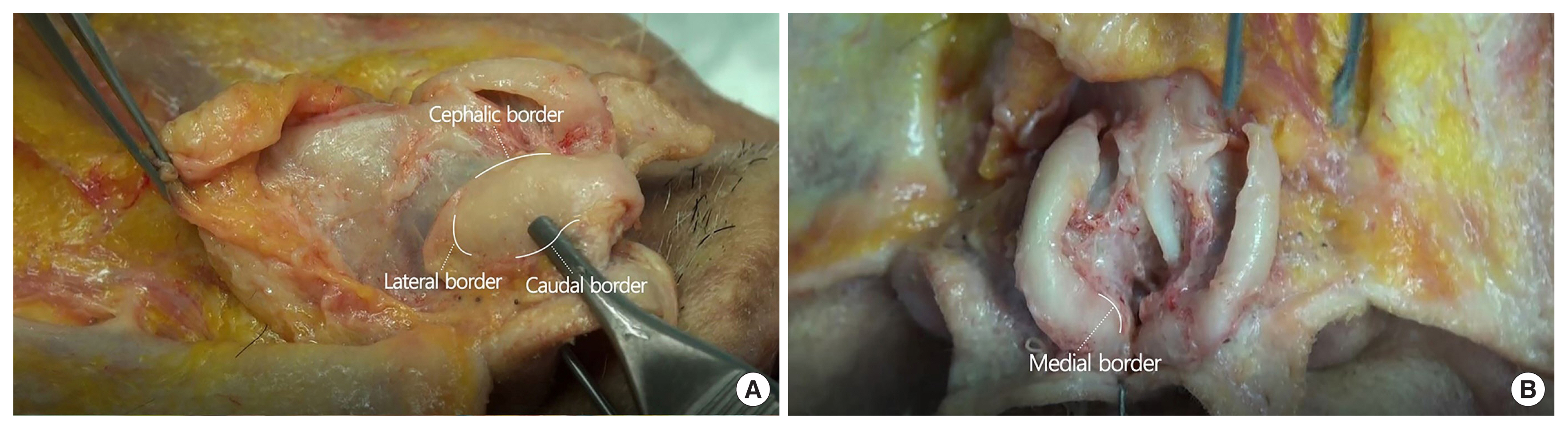
The alar cartilage can be divided into three parts: the lateral, middle (intermediate), and medial crura (Fig. 2). The lateral crus is a factor determining the antero-superior alar shape. It begins at the domal junction and ends at its junction with the accessory cartilages. It is connected to the pyriform aperture with a bridge of accessory cartilages [2ŌĆō5]. As described by Toriumi and Johnson [6] the lateral crus has a transverse (horizontal) and a vertical axis, and the shape of the lateral crus can be classified using the convex-smooth-concave configuration suggested by Zelnik and Gingrass [5]. Daniel et al. [7] later modified this classification with five different shapes according to a more detailed analysis of the configuration based on a cadaveric study: (1) smooth-straight, (2) convex, (3) concave, (4) smooth-convex, and (5) convex-concave-convex in the transverse axis (Fig. 3). These factors directly affect the position, shape, and volume of the nasal tip. The lateral crus has four borders: medial, lateral, caudal, and cephalic (Fig. 4). The medial border starts at the domal junction with the domal segment of the middle crus. The cephalic border of the lateral crus has an S-shaped scroll junction with the upper lateral cartilage. Since the alar cartilage is connected to the upper lateral cartilage through the scroll ligament, the mobility of the lateral crus plays a role in the functions of the internal nasal valve. The actual scroll area can vary from this common S-shape to an inverted, under-riding pattern. The S-shaped junction commonly contains small, fusiform, intervening sesamoid cartilages becoming isolated in juxtaposition to the mucosal space [8]. Although the caudal border often parallels the nostril rim before turning cephalically at the turning point of the lateral crus, it is quite often located cephalically away from the nostril rim because the alar cartilage is relatively narrow in Asian noses.
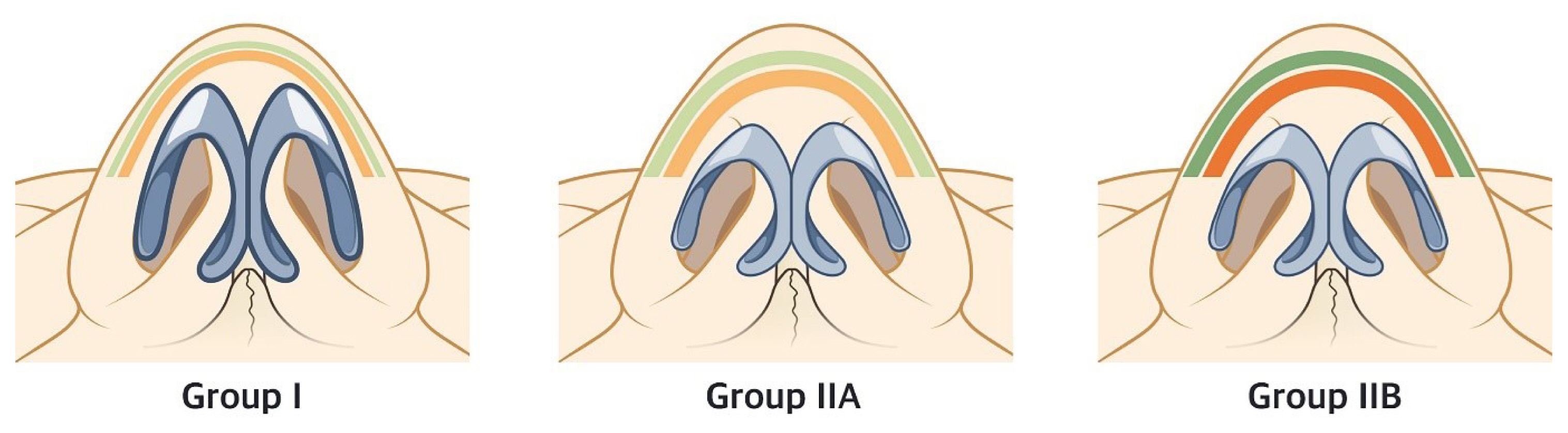
The middle crus begins at the columellar-lobular junction and ends at the lateral crus. It can be divided into lobular and domal segments [9]. The lobular segment plays an important role in shaping the lobule. It can often be identified exteriorly, although it may present as mismatched due to a thick nasal envelope or underdeveloped cartilage in Asians. The angle between both domes is called the angle of domal divergence. The nasal tip can be classified into three categories by divergence, as follows: a broad tip is one with more than 60┬░ of divergence, a boxy tip is one with wide divergence along with a wide domal segment (more than 4 mm), and a bulbous tip is one with wide divergence along with a rounded and ill-defined domal segment [10]. However, it is better to modify these definitions for Asian noses since the thick nasal envelope in Asians camouflages the classification of the nasal tip. Furthermore, the condition of the nasal superficial musculoaponeurotic system (SMAS), which is a main component of the nasal envelope, can affect how to correct a bulbous tip. The authorsŌĆÖ previous article introduced a classification for bulbous tips in Asians (groups I, IIA, and IIB) based on the etiology. Each group differs in terms of the characteristics of the SMAS reflecting onto the skin (Fig. 5) [11].
The medial crus is the primary component of the columella and can be divided into the footplate and columellar segment. The columellar breakpoint is affected by the width of alar cartilage and the pattern of the membranous and caudal septum, which seems to be less defined in Asians. Based on our experiences, there are cases where underdevelopment of the columellar segment causes a retracted columella along with a short and wide columellar base. However, underdevelopment of the footplate directly affects the shape of the columellar base and nostril [12].
Characteristics of the alar cartilage in Asians
Based on our own experience, the middle crus is usually underdeveloped in Asian patients. In particular, the domal segment of the middle crus is often weak and narrow. The shape and configuration of the lobular segment are also not clear in many cases. The major causes of under-projection in Asian nasal tip are weakness and underdevelopment of the footplate in the medial crus, which are also related to an acute nasolabial angle and retracted columella. In short, the underdevelopment of the middle and medial crura in Asians is the main cause of columellar retraction, wide round nostrils, lobular volume deficiency, and flatness of the columellar lobular angle in Asian noses [1].
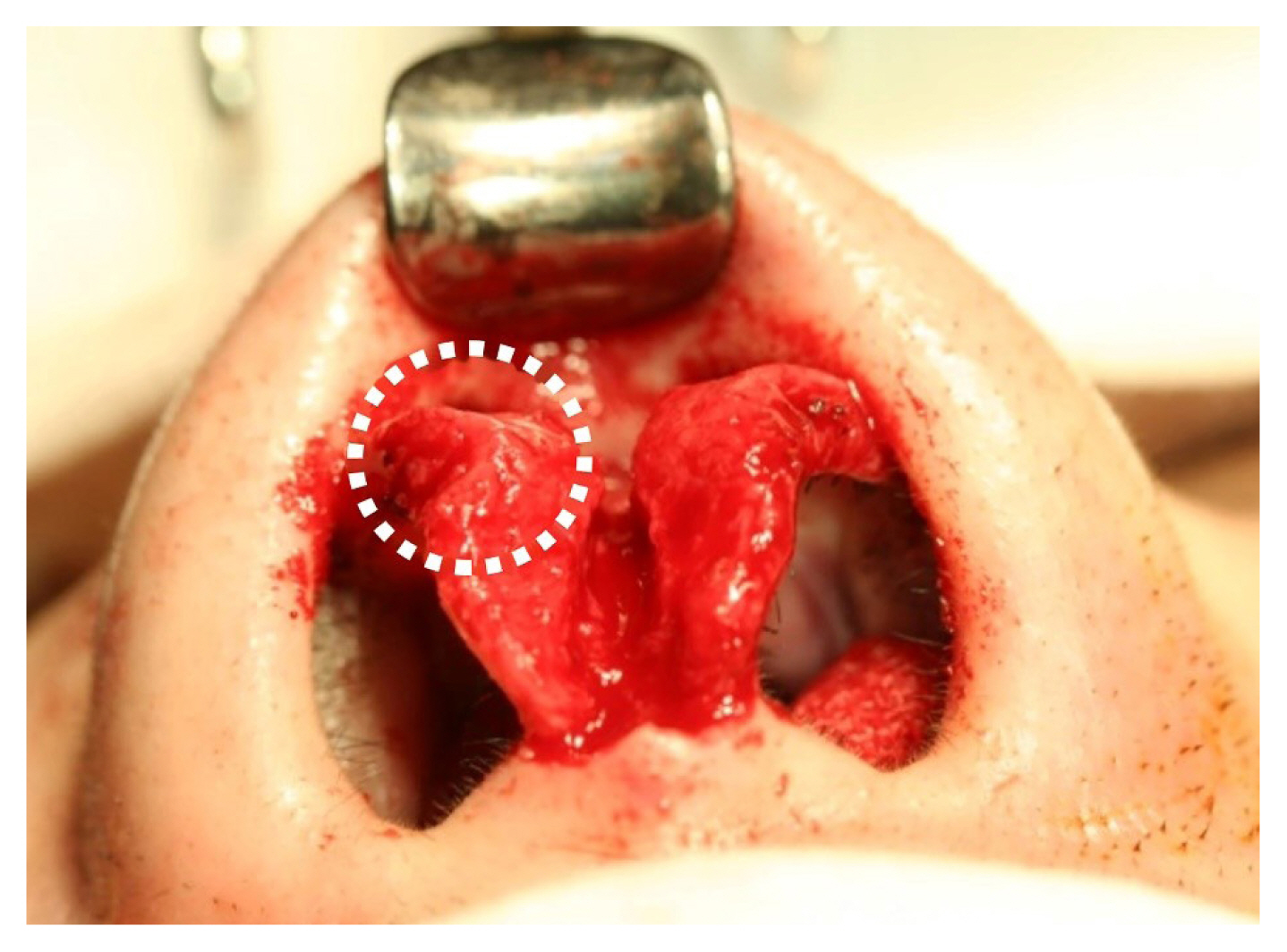
The alar cartilage in Asians in general has the following characteristics: (1) the borderline between the segment and junction in the alar cartilage is relatively obscure; (2) the angle providing definition between the domes is relatively wide; (3) the tip looks broad and under-projected because the border and axis of the lateral crus affect it; (4) the medial crus is short and less developed; (5) the footplate of the medial crus is short and loosely connected to the septum with fibrous tissue; or (6) medial curling of the middle crus is frequently observed (Fig. 6).
Nasal tip-supporting structures
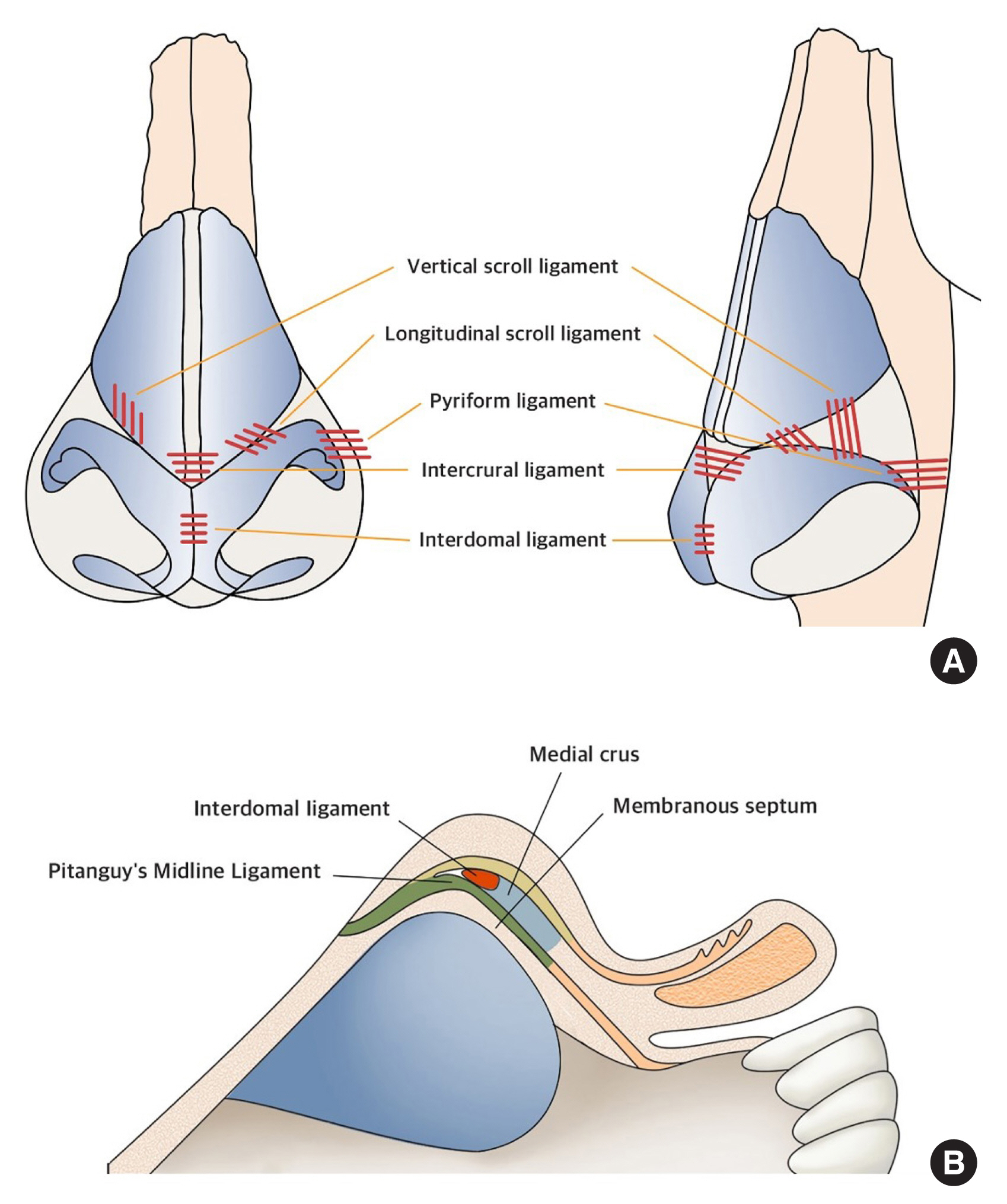
A successful result in Asian rhinoplasty depends strongly upon the management of tip-supporting structures by proper release of dense ligamentous attachments based on a thorough understanding of the tip-supporting structures, followed by refined suture techniques and cartilage grafts. The supportive structures of the nasal tip include the following [13]: (1) the scroll ligament: the structure between the upper lateral and alar cartilages; (2) the nasal hinge area (pyriform ligament): the composite tissue between the lateral crus and the pyriform aperture; (3) interdomal fat or loose connective tissue; (4) intervening structures between the medial crura and caudal septum, including the membranous septum; (5) the dermo-cartilaginous ligament (Pitanguy ligament); (6) the interdomal ligament (suspensory ligament); and (7) the intercrural ligament (Fig. 7).
Scroll ligament (longitudinal and vertical)
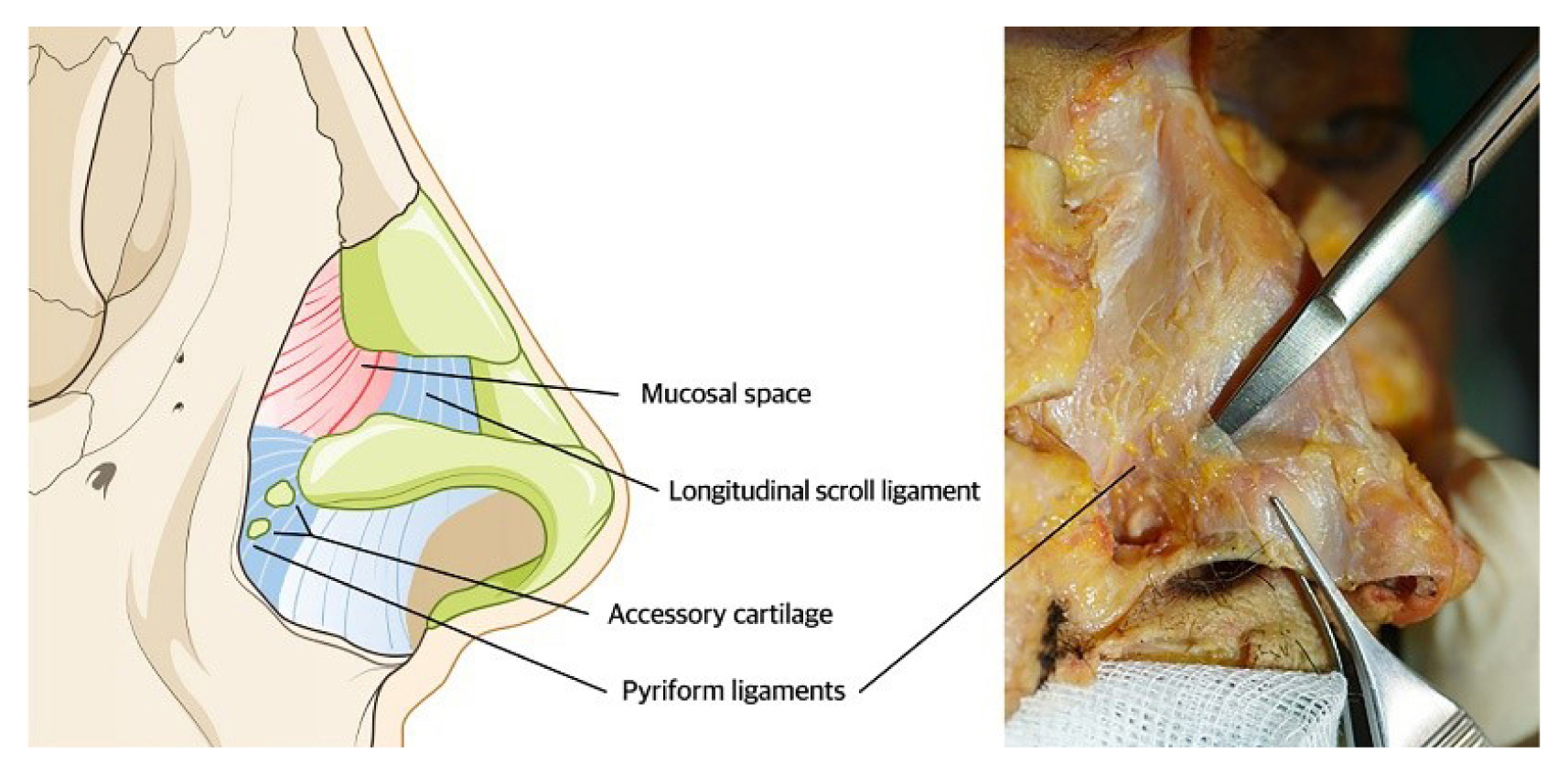
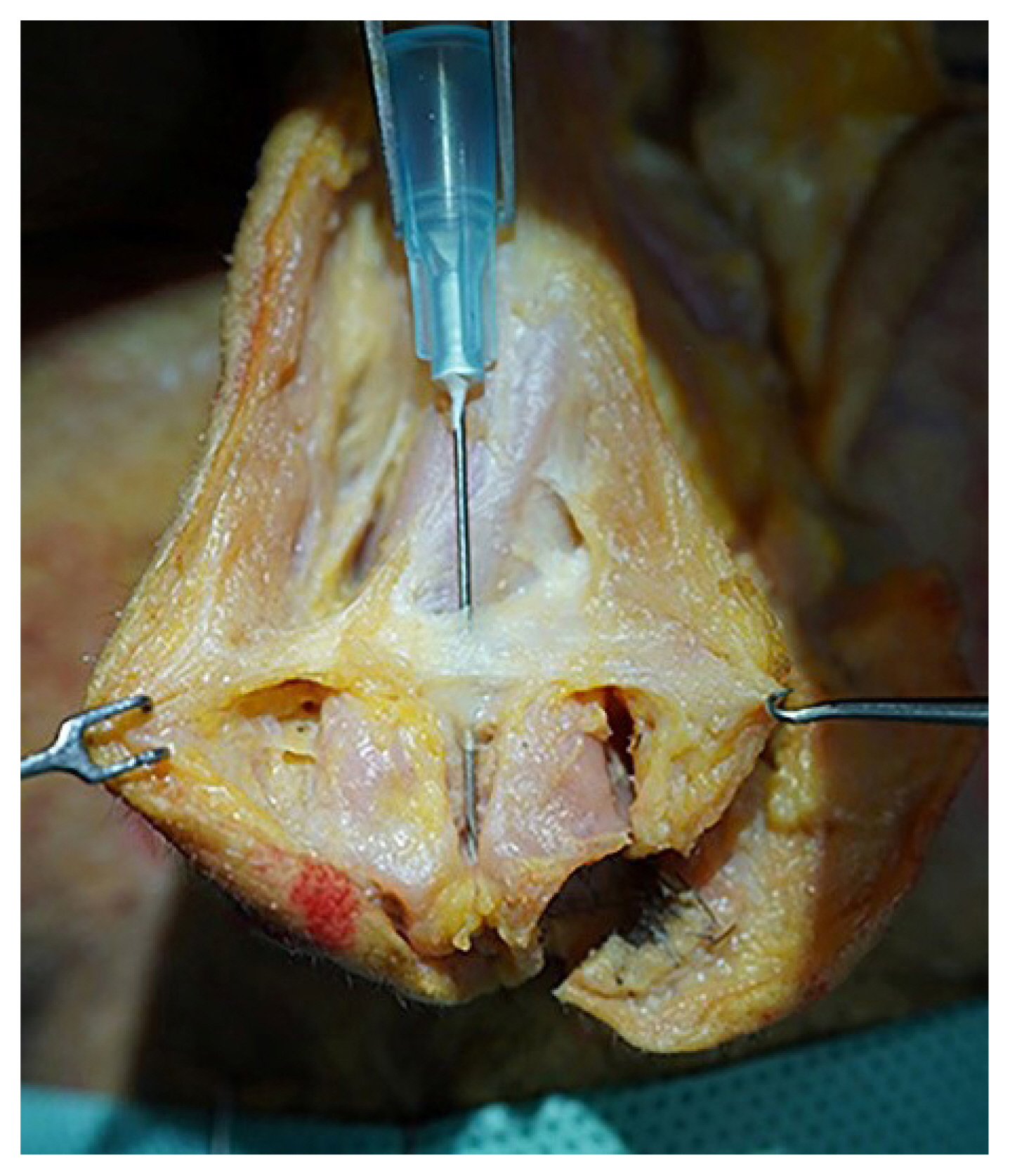
In Asian rhinoplasty, the scroll ligament is the most critical structure to understand the basic principle of advancement and pivot motion of the alar cartilage, since this surgical concept is frequently applied to inter-cartilaginous grafts, de-rotation grafts, and tip extension sutures. Therefore, adequate separation of the scroll ligament is the most important element to make alar cartilage free to be repositioned in specific cases, such as patients with an under-projected tip, drooping tip, and short nose [14]. It is an especially important structure in Asian rhinoplasty since more projection and lengthening of the tip is generally required than in Caucasian rhinoplasty (Fig. 8).
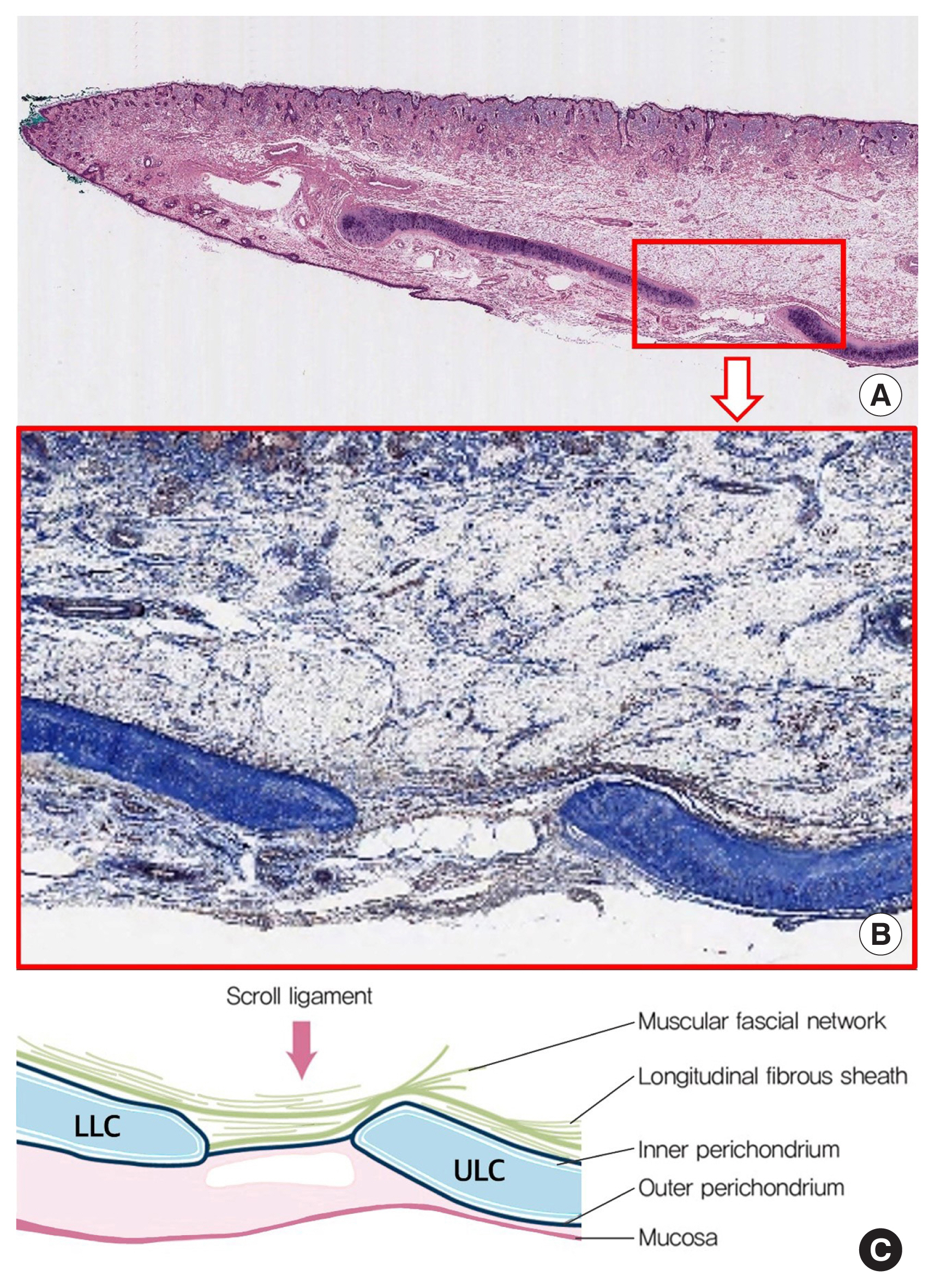
The scroll ligament embryologically starts to grow into the cartilaginous nasal capsule from connective tissues 6 months before birth. It further overlaps in the scroll configuration because the lateral crus of the alar cartilage is pulled above the upper lateral cartilage by tension during fetal development. The degree of curling depends on the strength of tension [15]. The ligamentous structures covering the scroll area have been described by many authors, although sometimes these structures have been identified as being part of the pyriform ligament. According to the authorsŌĆÖ cadaveric study and literature review, this structure is considered to constitute a combination of muscular fascial condensation with perichondrium or fibrosis of cartilage. The scroll ligament is not a separate structure connecting the upper lateral cartilage and alar cartilage in an end-to-end pattern, but a longitudinal fibrous sheath, a combination of periosteum and perichondrium descending caudally while covering the upper lateral cartilage and then finally wrapping above and beneath the alar cartilage (Fig. 9) [16]. Therefore, our previous study showed that it is appropriate to name this structure as the scroll ligament from a surgical view or as an inter-cartilaginous ligament from an anatomic perspective [17].
In a recent study, Saban et al. [18] identified a distinct fibrous attachment from the undersurface of the transverse nasalis muscles to the scroll junction. They introduced the concept of a vertical scroll ligament that emerges from the undersurface of the deep SMAS layer and inserts into the internal nasal valve area. Based on that, Daniel [19, 20] divided the scroll ligament into two structures, the longitudinal and vertical scroll ligament (Fig. 10). The longitudinal scroll ligament is a component of the ŌĆ£scroll complex,ŌĆØ which is generally called the scroll ligament. Anatomical studies have shown that the junction between the lower lateral cartilage and upper lateral cartilage has interspersed sesamoid cartilages within the fibrous tissue [19,20].
Nasal hinge complex with the pyriform ligament
In 1994, Adamson and Morrow [2] defined the nasal hinge as the most lateral portion of the alar cartilage. An accessory cartilage is firmly attached to the pyriform aperture at the nasal hinge by a ligament, fibrous tissue, and sesamoid cartilage. Various muscular fibers of the nasal periphery attach the lateral part of alar cartilage and the upper lateral cartilage at the nasal hinge. Moreover, three musclesŌĆöthe procerus, transverse nasalis, and levator labii superioris alaeque nasiŌĆöwithin the nasal SMAS restrain the lateral crus of alar cartilage from pivot motion and advancement. Since this area consists of muscle, fibrous tissue, the lateral crus, sesamoid cartilage, perichondrium, and fascia, it can be referred to as the nasal hinge complex. In our previous study, a longitudinal fibrous sheath formed by fusion of the periosteum and perichondrium, similar to the scroll ligament, was found to cover the upper lateral cartilage and wrap above and beneath the lateral crus of the alar cartilage and the accessory cartilage toward the pyriform aperture. Therefore, dissection should be performed on the supraperichondrial or subperichondrial plane of the alar and upper lateral cartilage since a lateral nasal artery responsible for nasal tip circulation and a superior alar branch of the facial artery run within or below the muscular layer (Fig. 11).
The pyriform ligament, first named by Rohrich et al. in 2008 [21], is a fascial support between the bones of the pyriform aperture and the adjacent cartilages (Fig. 12). It has been referred to using various other names, such as the lateral sesamoid complex ligament, lateral crural complex, and nasal hinge. The pyriform ligament can be understood as a wide fascial network system from the nasal bone down to the anterior nasal spine, providing static support for the nasal tip, alar base, and nasal vault [21]. A distinctive ligament was found, stretching from the second accessory cartilage to the pyriform aperture [7]. Furthermore, it reinforces the mucosal space as a dynamic structure, which is related to lateral wall insufficiency [22].
Aside from the pyriform ligament, Saban et al. [18] designated the ŌĆ£pyriform aperture ligament,ŌĆØ also called the ŌĆ£vertical pyriform ligament,ŌĆØ as a vertical attachment between the entire pyriform aperture and the overlying skin-soft tissue envelope. It is particularly dense over the keystone area and occasionally along the lateral border of the pyriform aperture [22]. Based on our cadaveric study, this ligament seems to be fused with transverse nasalis aponeurotic fibers, which the authors have introduced, makes dense structures above the osteo-cartilaginous junction, not at the margin of the pyriform aperture (Fig. 13). Further studies should be added to define this dorsal ligamentous structure and its margins as well [15,23]. Release of these complex ligamentous structures becomes an important surgical sequence during the dorsal exposure associated with hump correction, osteotomy procedures, or dorsal onlay grafts in Asian noses.
Dermo-cartilaginous ligament
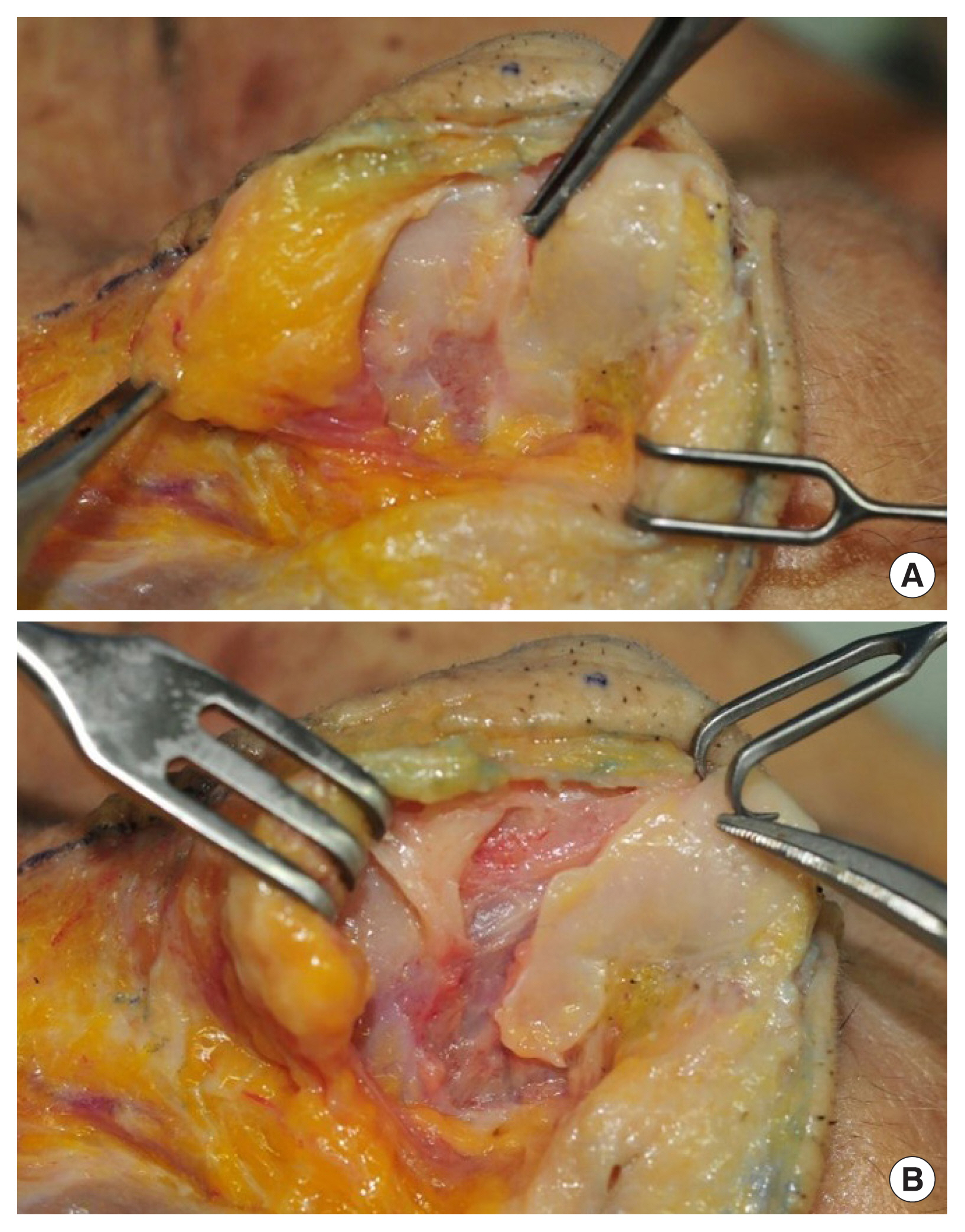
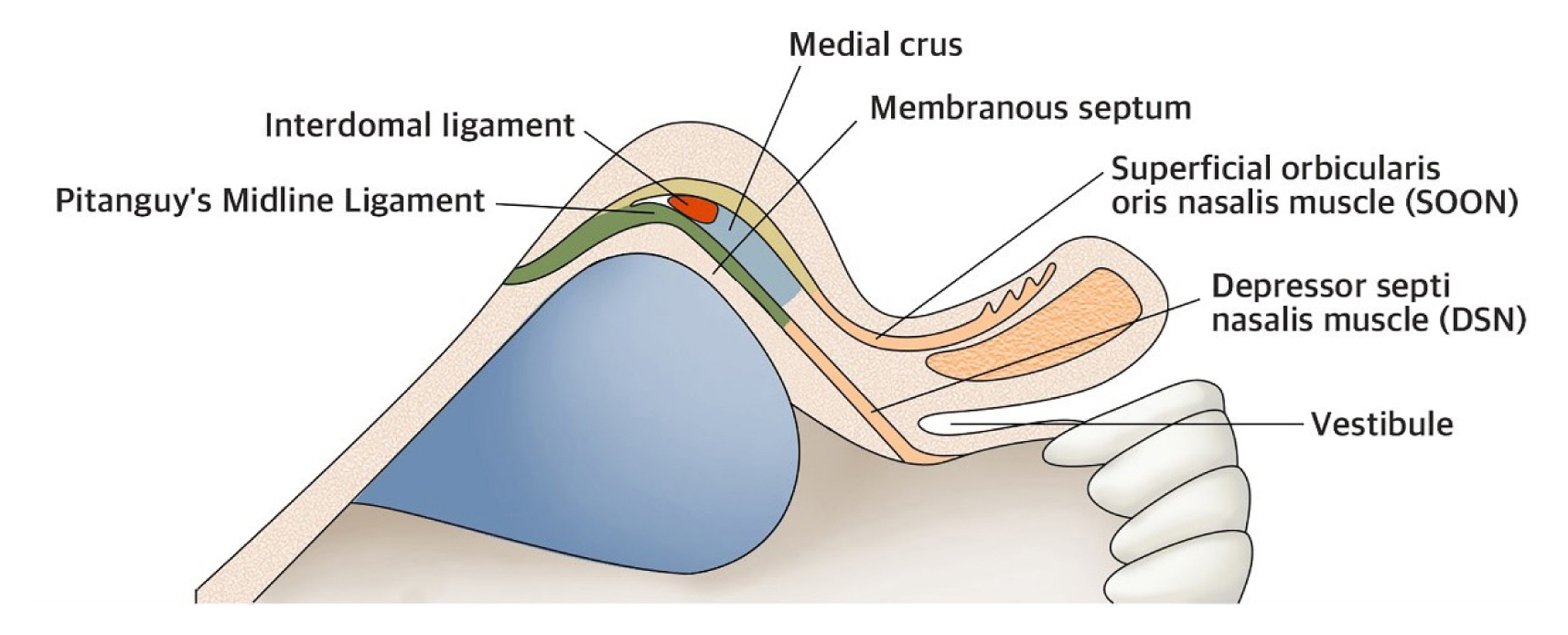
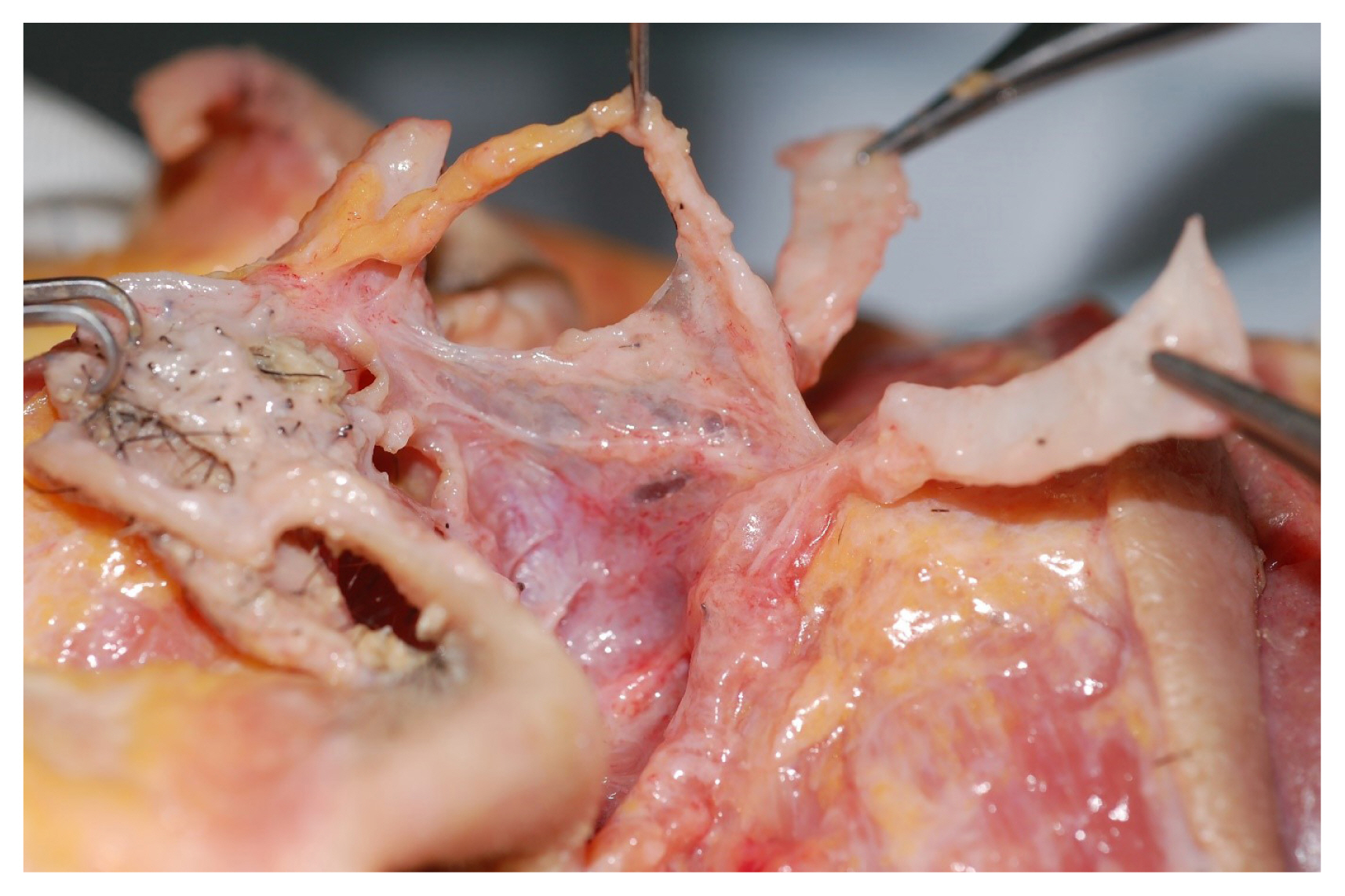
Pitanguy described a ligament originating from the undersurface of the dermis within the dorsal envelope, descending to and in between the alar cartilages tangentially and connecting to the depressor septi nasi [24,25]. Han et al. [26] suggested that the dermo-cartilaginous ligament should be renamed as the ŌĆ£median musculo-cartilaginous fascia,ŌĆØ since it is an independent structure having fascia with irregularly arranged connective tissue confirmed under microscopy and the dermo-cartilaginous ligament is considered to be a caudal extension of the distal nasal SMAS. Saban et al. [18] recently demonstrated that the medial SMAS at the level of the internal nasal valve divides into a superficial layer and a deep layer. They also modified the original terminology to ŌĆ£PitanguyŌĆÖs midline ligamentŌĆØ since it originates from the midline SMAS layer [27]. According to their findings, a superficial layer passing above the interdomal ligament becomes continuous with the superficial orbicularis oris nasalis muscle, and a deep layer passing below the interdomal ligament and becomes continuous with the depressor septi nasi muscle (Fig. 14) [22]. Although resection of the dermo-cartilaginous ligament improves nasal tip drooping, direct manipulation of the medial and intermediate fascicles of the depressor septi nasi that are attached to the dermo-cartilaginous ligament, septum and orbicularis oris, is necessary in cases of severe dynamic tip drooping. A connection between the dermo-cartilaginous ligament and depressor septi nasi was also confirmed in the authorsŌĆÖ study (Fig. 15) [28].
Interdomal ligament (interalar ligament, suspensory ligament)
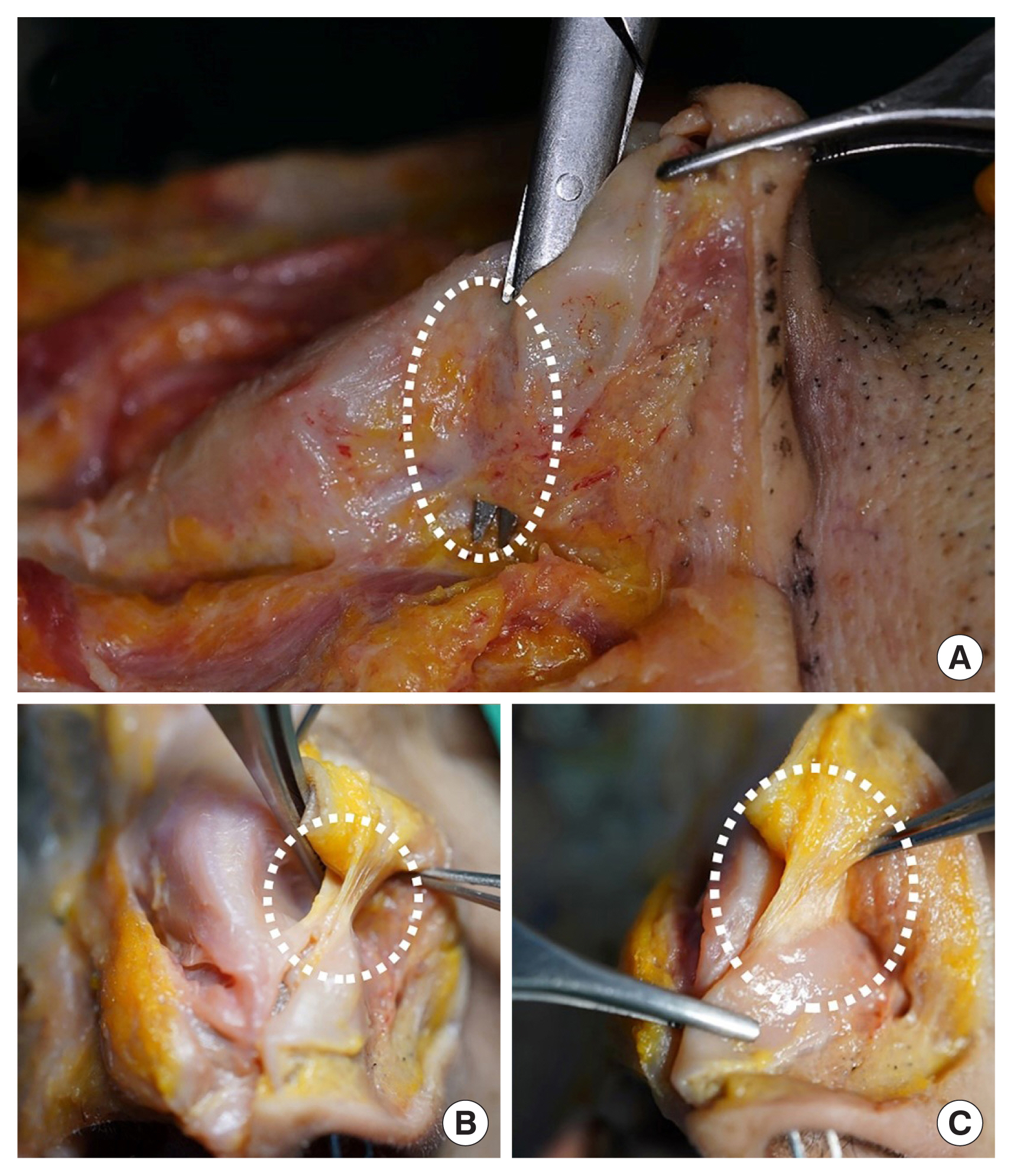
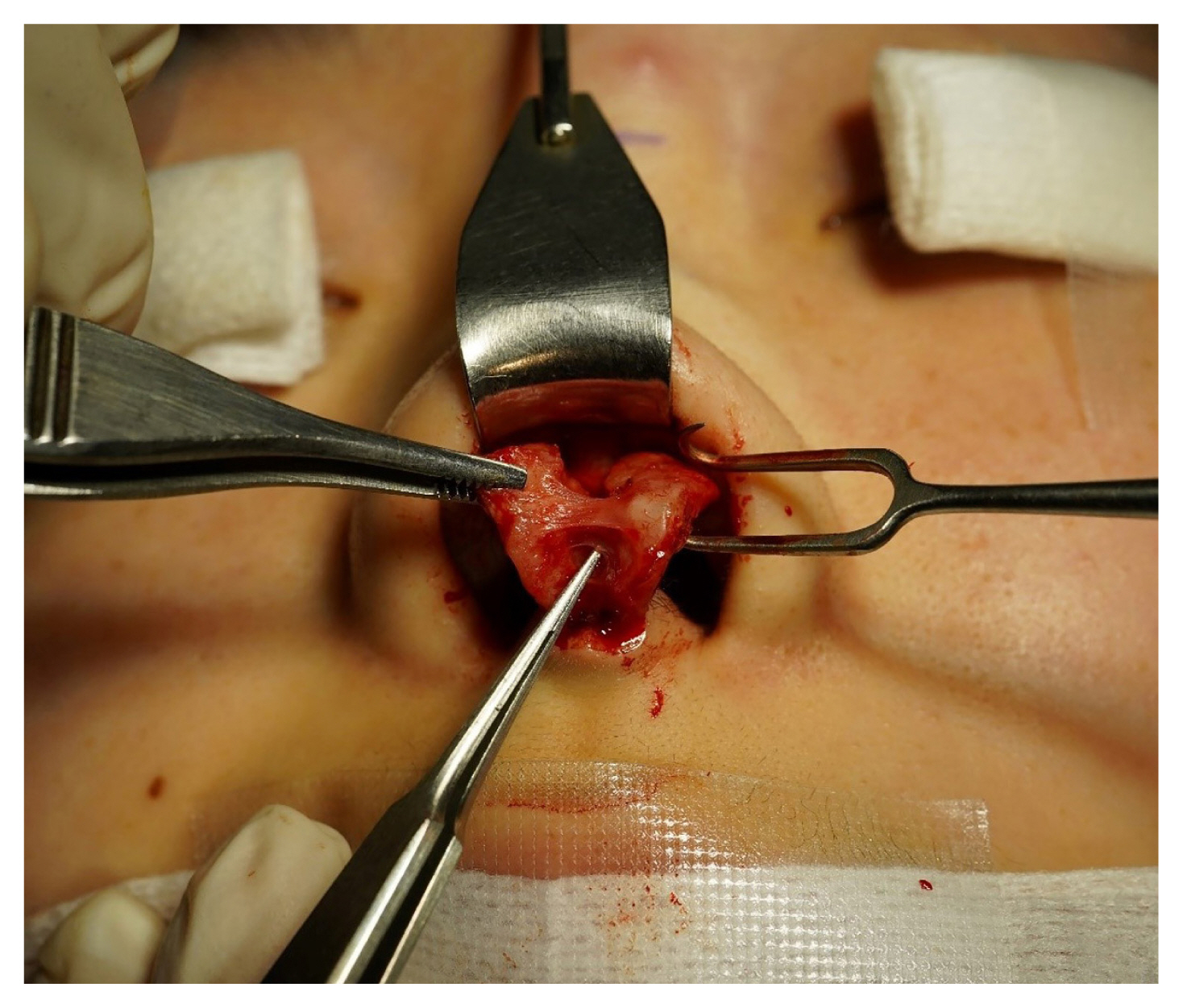
The interdomal ligament is a suspensory ligament connecting the medial borders of the lateral crura in the alar cartilage (Fig. 16) [29]. This ligament does not run between the domes, but rather more posteriorly and cephalically between the middle crura [22,30]. It shows wide variation, from barely visible to quite dense, among Asians. Although many surgeons cut it during the insertion of a columellar strut, the interdomal ligament can be easily preserved due to its cephalic position away from the caudal border of the middle crura. Obviously, this preservation is not possible if a tip split procedure is performed [30]. It is usually cut and reattached by suture techniques during tip plasty in Asian rhinoplasty (Fig. 17).
Intercrural ligament
The intercrural ligament connects the cephalic border of the entire alar cartilage, including the lateral, middle, and medial crura (Fig. 18) [22]. It passes just above the mucosa and holds the alar cartilage together. In its cephalic portion along the lateral crus, it acts as the suspensory ligament of converse passing just above the anterior septal angle. In its midportion, it is posterior to both the interdomal ligament and the deep portion of PitanguyŌĆÖs midline ligament [17]. Its caudal component effectively restrains the medial crus and footplate, pulling them toward the caudal septum. The intercrural ligament unifies the two alar cartilages and acts as a suspensory sling over the anterior septum. During rhinoplasty, this ligament can either be preserved or disrupted. In an open approach, a ŌĆ£tip splitŌĆØ procedure divides the ligament and requires the surgeon to restore support, usually with a columellar strut. However, downward traction on the alar cartilage followed by a ŌĆ£dorsal splitŌĆØ allows one to maintain the intercrural ligament. A bilateral transfixion incision through the membranous septum disrupts the intercrural ligament support between the footplates [22].
CONCLUSION
The anatomy of Asian nose is quite different from Caucasian one in characteristics of skin, bone, and cartilage. In addition, the surgical purpose and direction of Asian rhinoplasty are different from Caucasian rhinoplasty. Therefore, it is important to review surgical anatomy from the viewpoint of an Asian rhinoplasty surgeon to get the best result in practice.