

INTRODUCTION
Unilateral cleft lip is a complex congenital anomaly that occurs when the upper lip and nasal structures fail to fuse during embryonic development. This defect affects not only the facial appearance but also the function of the lip, nose, and maxilla. Surgical correction of cleft lip is usually performed in infancy to restore the normal anatomy and functionality of the affected structures, as well as to enhance the psychological and social well-being of both the patient and their family. Surgical repair of unilateral cleft lip is typically performed within the first few months of life to improve facial appearance and function and to prevent social stigma and psychological distress. The goal of surgery is to achieve a symmetric, functional, and esthetically pleasing lip contour, vermilion border, and nasal structure. Surgical techniques for unilateral cleft lip repair have evolved significantly over the past few decades, and the current approach is based on a combination of individualized planning, careful tissue manipulation, and meticulous surgical technique. Historically, several techniques have been developed for cleft lip repair, including the Millard rotation-advancement technique, Tennison-Randall technique, and triangular flap technique [1-4]. Each technique has its advantages and disadvantages, and the choice of technique depends on the severity and complexity of the cleft, the surgeonās experience and preference, and the patientās individual characteristics and goals. In recent years, several advances have been made in the field of cleft lip repair, including new surgical techniques and approaches. This review provides an overview of the current concepts and surgical techniques in unilateral cleft lip repair.
ANATOMY RELATED TO UNILATERAL CLEFT LIP
In patients with cleft lip, it is crucial to restore the normal structure of the lips, necessitating a thorough understanding of their anatomical features. The upper lip consists of the vermilion and white lip, featuring keratinized epithelium in the front and non-keratinized oral mucosa in the back. The tubercle is the central part of the vermilion, while the vertical area extending to the nose is known as the philtrum. The philtrum is a structure created by the intersection of the orbicularis oris muscle and is bordered by two vertical pillars. The upper lip is divided into the vermilion and white lip by the vermilion border, and the hairless area that blends with the white color above this border is referred to as the white roll [5]. The orbicularis oris muscle serves two functions: retracting the lips using the surface layer of muscle fibers and closing the oral sphincter with the deeper layers of muscle fibers. At the marginal part of the vermilion, the orbicularis oris muscle becomes shallow and concave, helping to maintain the natural shape of the lips.
Depending on the extent of the cleft, various changes can occur in the skin, muscle layer, and internal skeleton. In a complete cleft lip, the muscle fibers of the orbicularis oris muscle in the outer lip segment run horizontally toward the midline, then rise along the edge of the cleft to attach to the nostril sill, alar base, and pyriform aperture. The orbicularis oris muscle fibers in the inner lip segment also converge toward the midline and either attach to the periosteum of the upper jawbone at the alar base or become discontinuous in the subcutaneous tissue layer at the philtrum. In an incomplete cleft lip, if there is an absence of a skin bridge that is approximately one-third the length of the upper lip, the orbicularis oris muscle fibers in the outer and inner lip segments may not be continuous. Although a microform cleft lip has skin continuity, the continuity of the muscle layer beneath the skin groove may be disrupted.
The skin of the philtrum lacks hair and sweat glands. The red lips converge in an area where the lip segments split, and the lips are generally narrow on the inside and either wider or narrower on the outside. Regarding blood supply, the superior labial artery runs parallel to the fissureās edge in the outer lip segment and connects to either the angular artery or the lateral nasal artery. In the inner lip segment, the superior labial artery ascends through the fissure and connects to the posterior septal artery.
It is commonly believed that variations in unilateral cleft lip are present only on the affected side. However, a 2021 study by Tse et al. [6] demonstrated that variations exist on both sides. For example, in patients with unilateral cleft lip, the philtral area on the affected side is displaced to the opposite side, aligning with the position of the maxilla. Additionally, the alar base on the non-affected side is positioned more superiorly and laterally compared to the affected side. Consequently, when treating unilateral cleft lip, it is essential to consider deformities on both the affected and non-affected sides. Gaining an accurate understanding of the changes in the non-cleft side prior to surgery is crucial.
PRESURGICAL MANAGEMENT OF UNILATERAL CLEFT LIP REPAIR
Corrective surgery prior to unilateral cleft lip repair aims to minimize skeletal and soft tissue deformities, converting the cleft lip from a complete to an incomplete type. Common preoperative correction techniques include lip taping, silicone conformers, lip-nose adhesion, the Latham device, and nasoalveolar molding.
Lip taping and silicone conformers can be applied immediately after birth. Taping is applied to both cheeks to promote the fusion of separated segments and to decrease tension between tissues during primary surgery [7]. Silicone conformers take advantage of the plasticity of newborn cartilage to lift and reshape deformed nasal cartilage, and can be used in cases of incomplete clefts with nasal floor deficiency [8]. Lip-nose adhesion is another method for correcting incomplete cleft lip, typically performed before the age of 2 to 3 months [9]. This technique involves filling the gap in the upper lip and the cleft in the alveolus, effectively converting a complete cleft lip into an incomplete one. The position of the maxillary arch and nasal cartilage can be adjusted using a rectangular skin flap originating from the edges of the cleft. While this method can help reduce tissue tension before primary surgery, it is not commonly used due to the scarring and abnormal adhesion of the nose that may result from the surgery (Fig. 1).
The Latham device is an active preoperative orthopedic device used to correct unilateral cleft lip and palate [10,11]. It comprises an adjustable screw-type framework affixed to the maxillary arch, which serves to correct the premaxillaās displacement. This device is engineered to exert a gentle force that repositions the premaxilla to the midline and enhances the alignment of the alveolar ridges prior to primary lip surgery. The correction process entails weekly adjustments of the device by the childās caregiver, under the supervision of a medical professional. Although the Latham device has been deemed highly effective in ameliorating the alignment of the alveolar ridges and mitigating the severity of the cleft deformity, its usage has waned in recent years due to its potential impact on facial growth, particularly on maxillary development. Moreover, the implementation of the device necessitates a minor surgical procedure to fix it in place, which may cause discomfort and inconvenience for the child and their family.
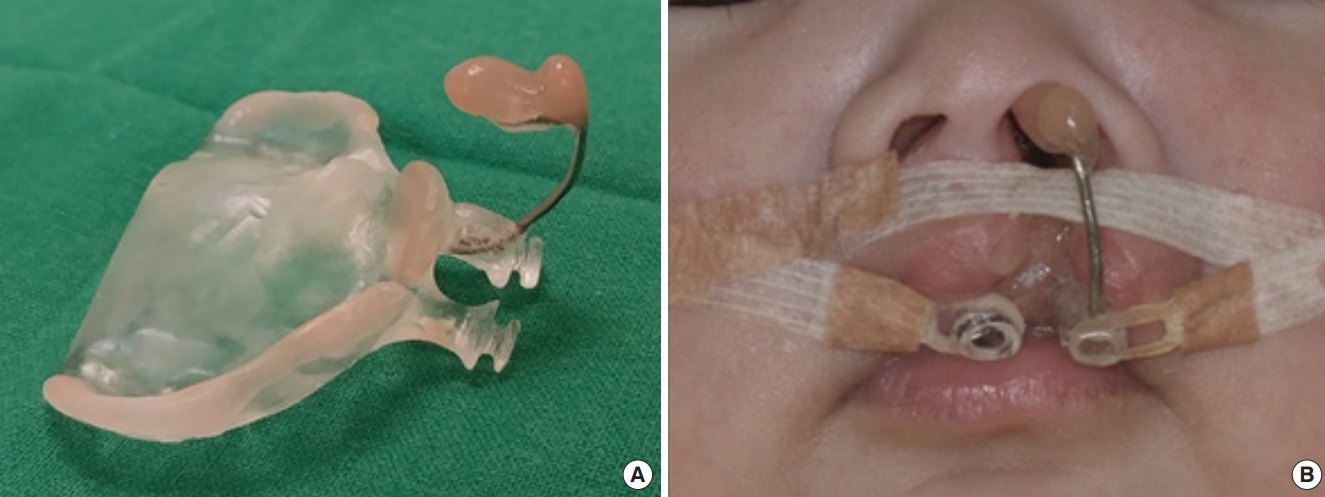
Nasoalveolar molding is a technique utilized for treating unilateral cleft lip and palate (Fig. 2). This method can lessen the severity of the cleft deformity, enhance the symmetry of the nose and lip, and reduce the necessity for extensive surgical intervention during primary repair. The technique involves the use of a custom-made oral appliance worn by the infant to preoperatively mold the nasal and alveolar structures. This appliance comprises a nasal stent and a plate that covers the cleft in the gum. Nasoalveolar molding treatment is typically initiated within the first few days following birth and continues until the primary lip repair, which is usually performed around 3 months of age. Studies have revealed that employing nasoalveolar molding can lead to improved esthetic outcomes and fewer surgical procedures for children with cleft lip and palate compared to other techniques [12,13]. However, it requires a high level of expertise from the healthcare team and commitment from the parents to follow the treatment protocol.
EVOLUTION OF SURGICAL TECHNIQUES: FROM HISTORICAL BEGINNINGS TO UP-TO-DATE CONCEPTS
Surgical treatments for unilateral cleft lip and palate aim to correct lip and nose deformities, restore symmetry, and promote normal midface growth in the long term. Patients present with a variety of anatomical deformities that necessitate individualized approaches. The size of the cleft and the presence of syndromes also impact the selection of surgical techniques. Regardless of the chosen surgical technique, the primary objective is to achieve equal lip height between the cleft and non-cleft sides. Numerous cleft lip and nose repair designs have been proposed by several prominent surgeons (Fig. 3).
The Tennison-Randall method
This method was invented by Tennison based on the Le Mesurier method and later refined by Randall et al. [1,2]. This method addresses the insufficient length of the inner lip segment by using a triangular flap from the outer lip segment to adjust the length. The white line of the outer lip segmentās vermilion is inserted into the back-cut of the white line of the inner lip segmentās vermilion, thereby adjusting its length. Therefore, a triangular scar may remain on the philtral area. To improve the continuity of the area and minimize deformity in the repair of unilateral cleft nose, Cronin [3] later suggested designing the triangular flap 1 mm above the red lip border.
Rotation-advancement technique: the Millard method
The Millard rotation-advancement technique follows the principle of removing minimal tissue and using as much tissue as possible for cleft correction [4]. This method involves advancing the outer cleft segment of the upper lip inward and rotating the inner lip segment downward, preserving both Cupidās bows and the philtrum. The tension from suturing is aligned along the vermilion border, preventing the scar from spreading outward. The surgical procedure entails designing a curved incision line on the inner lip segment from the highest point of the Cupidās bow to the base of the cleft, rotating the tissue downward from the cleft base, and performing a horizontal incision at the vermilion base of the outer cleft segment to advance it inward. Subsequently, various surgical methods have been proposed that involve modifications of the Millard technique.
The extended Mohler method
The extended Mohler method, a modification of the Millard method, is based on the principle of applying a mirror image of the normal sideās philtral distance to both the inner and outer cleft lip segments of the affected side [14]. The original Millard method had the disadvantage of widening the gap between the alveolar ridges and causing significant deformation of the upper part of the philtral segment when a large amount of rotation and advancement was required. Additionally, it reduced the size of the affected sideās cleft due to excessive advancement of the outer flap. In the extended Mohler method, the design at the upper part of the philtral segment differs from that of the Millard method, with the back-cut directed toward the non-lip side rather than toward the lip side at the non-commissural boundary, securing the length of the inner cleft lip segment. Thus, the Millard method improves the natural appearance of the philtral unit in the upper one-third of the philtral segment.
The Fisher anatomic subunit method
Fisher employed geometric principles to perform vermilion correction, which utilizes the anatomical subunits of the face [15]. The Fisher method uses 25 anatomical landmarks and depends exclusively on direct measurements. Initially, the total lip height, greater lip height, and lesser lip height are precisely measured using calipers. As per their respective definitions, the total lip height refers to the philtral column length on the non-cleft side, measured from the white roll to the vermilion border. The greater lip height is the distance from the white roll to the vermilion border of the inner lip when it is appropriately pulled down. Meanwhile, the lesser lip height is the width of the triangular skin graft at the vermilion border of the outer lip. Mathematically, the lesser lip height can be determined by subtracting the greater lip height from the total lip height and adding 1 mm, which accounts for the Rose-Thompson effect, where the curved part is straightened and lengthened. Moreover, the position of the point placed on the outer lip segment varies depending on the height of the outer lip segment and the severity of the vermilion discrepancy.
Curved-line cheiloplasty: the TS Oh method
Although various methods of cleft lip repair have been previously described, offering advantages such as the creation of natural-looking philtral scars and restoration of symmetry, they also present several limitations. Millardās rotation-advancement method may result in the sacrifice of mucosal and lip tissue when excessive tissue rotation and advancement are performed in cases with a short vertical height of the outer lip segment. To overcome this disadvantage, Mohler extended the incision line primarily toward the nasal side, Onizuka created a small triangular flap in the vermilion area to reduce the back-cut amount, and Noordhoff omitted the extension incision at the base of the cleft. The Fisher method, in contrast, involves a relatively higher amount of tissue loss due to its straight-line design, which may result in excessive excision in cases with a short vertical height of the outer lip segment. The author has developed a curved-line design to minimize tissue loss and achieve optimal symmetry by addressing the disadvantages of existing methods [16].
This method effectively minimizes tissue loss, particularly when there is insufficient tissue in the outer lip segment or a large gap in the vermilion border. By using a wire to create a curved template, the natural curves of the philtral column can be fully restored. Noordhoff ās point, also known as CPHLā, is designed at the thickest part of the philtral area, which then tapers off. However, many surgeons face difficulties in accurately drawing this point, as the curveās shape varies depending on the patient, and the thickness of the philtrum may remain constant or become thinner towards the upper part. To address this, the author used a wire to ensure symmetry in the vertical length of the upper lip and consistently located the CPHLās point. When employing this method, the CPHLās point is often drawn outward compared to the traditional Noordhoff ās point, potentially causing asymmetry in the horizontal length of the outer lip segment. However, based on the authorsā experience, asymmetry in the horizontal length of the upper lip is less noticeable than asymmetry in the vertical length, and the results are frequently more aesthetically pleasing.
Surgical techniques based on the curved-line cheiloplasty method
Anthropometry and design
Before surgery, the Cupidās bow points (CPHR and CPHL), white roll, labiale superius, highest points of the philtral column (CPHSR and CPHSL), bilateral base of the ala (SBAR and SBAL), and commissures (CHR and CHL) are marked (Fig. 4) [17]. In curved-line cheiloplasty, three-dimensional matching of the non-cleft side philtrum is attempted using a flexible wire [16]. First, the length from the nasal sill to the highest point of the Cupidās bow on the non-cleft side (length āaā) is measured and marked on the wire. Taking into account the contour of the orbicularis oris muscle, point O is marked on the wire and aligned with point B on the columellar base. The lowest point of the wire is marked as point K, which is length ābā away from point O. Length ābā is 2 mm shorter than length āaā due to the Rose-Thompson and triangular flap effects [18]. Point K is matched with point A on the Cupidās peak on the non-cleft side. To allow adequate rotation, a back-cut is made on the white skin roll on the non-cleft side. A 1-mm triangular flap from the cleft side is used to repair the defect, which also helps to elongate the cleft-side tissue and revise the stigma. This flap is employed for controlling the position of Cupidās peak. Curved-line cheiloplasty mimics the philtral column length using a flexible wire and introduces new landmark points O and K, representing the upper and lower margins of the reconstructed philtral column on the cleft side, respectively. Reconstructing the disrupted continuity is more effective in restoring the original curve on the cleft side than relying on the conventional straight-line method (Fig. 5).
Incisions
Separate incisions are performed in the outer and inner lip segments. In the outer segment, the incision follows the curved line drawn with a wire, extending from point K to point O, in order to elevate the L flap. A 1-mm triangular flap is subsequently elevated at the superior aspect of the white roll. It is crucial to preserve the white roll, as damage to it may result in an unnatural appearance of the lip border. Next, the mucosal flap is elevated at the vermilion border by vertically traversing the vermilion and utilizing the junction of the dry and wet vermilion as the apex of the vermilion triangular flap. The incision then proceeds vertically downward to the level of the alveolar crest, forming the base of the L flap.
The incision at the medial lip segment follows the standard rotation-advancement technique. It begins at the CPHL and curves outward towards the CPHSL before extending horizontally along the columellar base. To avoid excessive scarring, the incision should not surpass half the width of the columellar base. Next, an incision is made from the CPHL along the mucocutaneous junction to its highest point, forming the C flap. The inner incision of the C flap extends 2 to 3 mm towards the septum, predicting the nostril sillās location. Subsequently, the incision is extended vertically from the CPHR to the alveolar crest, creating the M flap. Back-cuts are made in the upper portion of the white roll and at the vermilion border between the dry and wet mucosa. Additionally, a sulcus flap (S flap) is formed at the base where the inner lip split meets the alveolar bone, reconstructing the mouthās vestibule (Fig. 6).
Muscle dissection
Muscle dissection is performed by elevating the subcutaneous layer and dissecting the muscle both superficially and deeply by 2 to 3 mm. In the outer lip segment, the orbicularis oris and levator anguli oris muscles may be abnormally attached to the maxilla, necessitating the release of any adhesions between the bone and muscles. The extent of muscle dissection in the inner lip segment depends on the degree of lip rotation required. Over-dissection may result in challenges recreating the concave shape of the philtral dimple. Detaching the periosteum from the base of the maxilla enables unrestricted movement of the outer lip segment. The periosteal detachment should be carried out in the pre-periosteal plane and continued until the orbital floor is exposed in the upper portion. Following the detachment, the muscle should be repositioned inward to guarantee adequate detachment.
Septal repositioning
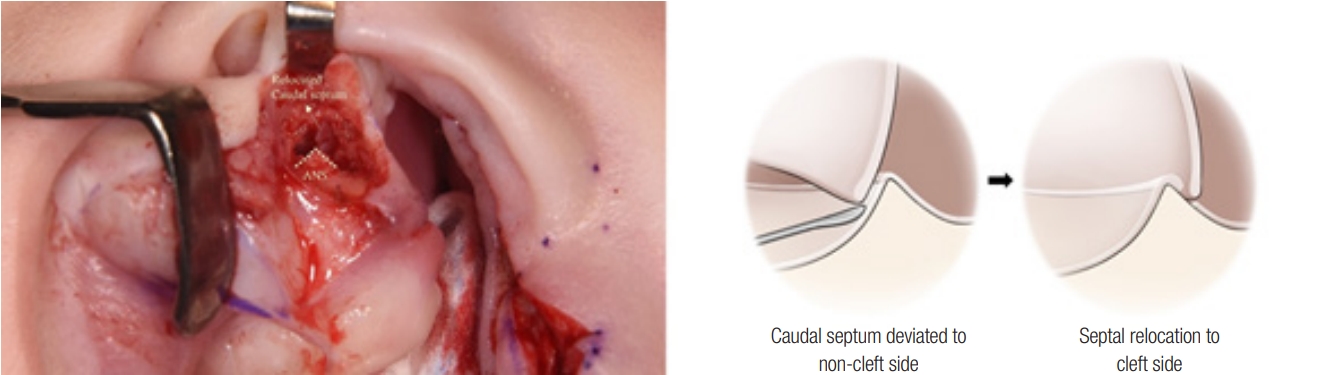
Dissection is performed downward beneath the C flap to expose the nasal septum and anterior ethmoid region. This procedure must be performed with caution to prevent damage to the sphenopalatine artery. In cases of a unilateral cleft palate, the nasal septum frequently deviates in the direction opposite to the cleft, and the anterior ethmoid region tends to shift in the opposite direction as well. The septospinal ligament, a robust ligamentous structure situated between the nasal septum and anterior ethmoid region, is dissected to separate the nasal septum from the anterior ethmoid region. Once separated, the nasal septum is repositioned toward the direction of the cleft (Fig. 7) [19].
Sulcus and nasal floor reconstruction
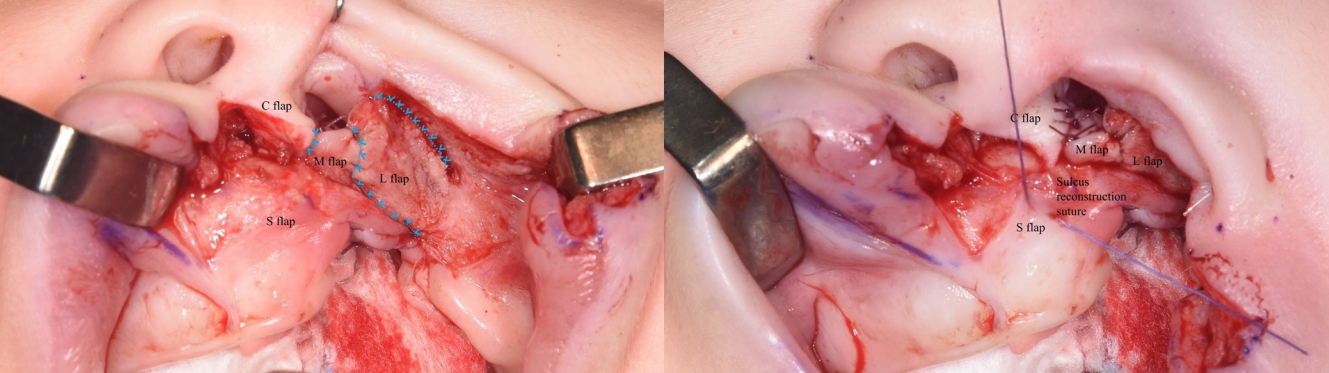
To reconstruct the oral sulcus, four flapsāthe L, M, C, and S flapsāare raised from the inner and outer labial segments. First, the end of the L flap on the vermilion side is sutured to the other end of the anteriorly placed L flap, creating the outer aspect of the oral sulcus. Next, the end of the M flap is sutured to the basal part of the L flap in a crossed manner, forming the inner aspect of the oral sulcus. The C flap is then rotated toward the nasal cavity and sutured, establishing a portion of the vestibule and providing support for the nasal floor. The S flap is sutured using the quilting method to maintain the depth of the oral vestibule and prevent obtuse sulcus angles. Finally, the outer labial segment is advanced inward to match the length of the inner labial segment, and suturing begins from the deepest part of the sulcus (Fig. 8).
Alar base medialization
The alar base of the external lip segments is sutured to the foot-plate region of the columellar base in the medial lip segment. Next, the uppermost portion of the orbicularis oris muscle in both the outer and inner lips is sutured together for reinforcement. The objective of the alar cinching suture is to overcorrect the alar base position by 1 to 2 mm upward and inward relative to the opposite position [13]. The movement of the orbicularis oris muscle should be directed inward, upward, and cranially to create an eversion of the upper lip contour (Fig. 9).
Orbicularis oris muscle reconstruction
The orbicularis oris muscle is reconstructed using an overlapping technique, where the outer orbicularis oris muscle covers the inner orbicularis oris muscle, increasing thickness from the outer area and recreating the shape of the lip column [21]. Muscle suturing is performed using a 4-0 Vicryl suture in a vertical mattress technique. To create a philtral dimple, the dermis layer of the inner lip segment is sutured to the muscle layer. Careful repair of the pars marginalis of the orbicularis oris muscle is essential to prevent flattened or retracted appearances after suturing (Fig. 10).
White roll reconstruction and skin repair
The triangular white roll flap plays a role in aligning the height of Cupidās bow and prevent it from rising postoperatively. To preserve the continuity of the white roll, the author designed a 1-mm triangular flap situated approximately 1 to 2 mm above the vermilion-cutaneous junction. During skin closure, the flap is inserted by executing a horizontal back-cut in the opposing white roll area [22]. The dimensions of the triangular flap are determined by the thickness and volume of the vermilion tubercle. Prior to skin closure, the appropriate degree of rotation is assessed, and any final adjustments are made. If excess tissue remains, the C flap can be trimmed. The incision at the nasal sill is closed using a 6-0 fast resorbing Vicryl suture, while the cutaneous layer of the upper lip is closed with a 7-0 nylon suture (Fig. 11). A representative case is presented in Fig. 12 [20].
PRIMARY CLEFT RHINOPLASTY: A REVIEW OF TECHNIQUES AND PROPOSALS
A previous study reported that over half of American cleft palate-craniofacial surgeons currently perform some form of primary nasal correction in patients with unilateral cleft lip [23]. However, the selection of appropriate techniques has been a topic of extensive debate, leading to significant variation in the timing, techniques, and extent of correction during cleft rhinoplasty [24-27]. Data on preferred techniques for primary cleft rhinoplasty reveal inconsistent management of the lower lateral cartilage [25]. Most surgeons reported consistently dissecting the alar cartilage, but only one-third of respondents relied on suture fixation of the alar cartilage. The challenges of manipulating infantile nasal cartilage, which is inherently thin and pliable, may deter surgeons from placing intercartilaginous sutures.
In primary cleft rhinoplasty, the alar cartilages are regarded as the crucial elements requiring correction. Berkeley was the first to suggest direct repositioning of the alar cartilages [28]. He accomplished this during primary labial repair by placing a horizontal mattress suture between the cartilages through an external skin incision [28]. McComb [29] is notable as a significant advocate for cartilage repositioning. He performed a more extensive correction of the nose by elevating the alar cartilage and shortening the cleft side hemi-nose. The scope of nasal skin dissection extended from the alar rim over the nasal tip and up to the nasion on the cleft side nose, without an intranasal incision. The alar cartilage was elevated by placing a long mattress suture between the nasal vestibule, through the intercrural angle and lateral crus, and up to the nasal skeleton at the nasion. This surgical technique for nasal dissection, alar elevation, and stabilization was embraced by proponents of primary nasal correction. Meanwhile, additional incisions, such as the reverse U, infracartilaginous, and intercartilaginous incisions, were employed to access the alar cartilages [17,30,31].
Several authors have reported new techniques for alar cartilage repositioning to facilitate procedures and enhance the accuracy of suspension. Kernahan et al. [32] performed primary rhinoplasty using modified Tajima methods and developed a Senn retractor with an open center to grasp a double-armed suture intranasally, placing it in the contralateral upper lateral cartilage [33]. This allowed the suture to be pulled out of the cleft side nostril when the retractor was withdrawn. Rottgers and Jiang [34] employed a hollow needle to place a suspension suture between the contralateral upper lateral cartilage and the cleft side lower lateral cartilage.
Cartilage correction surgery via a semi-open rhinoplasty involves the following steps: (1) employing a semi-open approach through an incision on the edge; (2) gently peeling the surface of the non-irritating cartilage; (3) suspending the dome area of the non-irritating cartilage for repositioning; and (4) threading a needle through the supralateral cartilage and then through the non-septum. At this point, the needle tip is pulled out until the marked section, allowing the suture material to be embedded. (5) After suturing the cartilage, the non-mucosal incision is stitched, and (6) quilting sutures are performed in the non-irritating and non-cartilaginous areas to ensure there is no dead space surrounding the non-irritating cartilage.
In a related context, the author introduced a novel surgical technique based on the semi-open rhinoplasty approach through a marginal incision in the cleft side nostril (Fig. 13). The authorās method employs a specially designed needle (Changās needle, HansBioMed Corp.) to simplify the placement of an intercartilaginous suture between the lower and upper lateral cartilages. Dissection extends across the nasal envelope overlying the dome of the alar cartilage and the nasal tip, creating space for the intercartilaginous suture. Using Changās needle with a 5-0 polypropylene thread, the dome of the alar cartilage is sutured, and the needle is directed medially and cranially, piercing through the septal and contralateral upper lateral cartilages. The needle is then withdrawn from the skin until the laser mark is visible and reinserted into the intranasal side. Subsequently, an intercartilaginous suture is performed along the cleft side alar cartilage, septal cartilage, and contralateral upper lateral cartilage. This technique enables stable fixation between the cartilages without extensive subcutaneous undermining, preventing scar contracture and preserving growth potential. Representative cases are illustrated in Figs. 14 and 15.
CONCLUSION
Contemporary techniques for unilateral cleft lip repair aim to achieve three-dimensional anatomic and functional restoration of the affected structures. Various cleft lip repair techniques have been proposed, with some relying on precise anatomic geometry, while others allow for greater flexibility in design. Primary cleft rhinoplasty is currently considered an optimal technique, targeting the deformed lower lateral cartilages, septum, and nostril floor. The primary cheiloplasty and rhinoplasty techniques we describe herein have evolved over time, based on our extensive experience and lessons learned from previous generations of cleft surgeons who pursued optimal results. To achieve the best outcomes, cleft surgeons must adopt a comprehensive approach, with meticulous preoperative planning to determine the most suitable surgical approach for each individual patient.